Metabolic Psychiatry
Weight, mood, sleep, and cardiometabolic risk should be read together.
Medication decisions are stronger when appetite, labs, lean mass, sleep apnea, mood, anxiety, and long-term risk are reviewed in the same plan.
Care path: metabolic and labs review
Best fit when mood, appetite, sleep, weight, lab patterns, and medication risk need to be considered in one clinical plan.
Available for appropriate patients in California and Arizona.
Not every article needs an appointment. Use this page for research. Turn it into a visit when the pattern is affecting a real medication, diagnosis, or daily-function decision.
Turn this into a visit when
- Mood, sleep, appetite, weight, labs, and medications are moving together.
- A GLP-1, stimulant, sleep issue, or metabolic change is affecting how you feel.
- You want the psychiatric plan to account for body data, not ignore it.
Bring this pattern
If this is the question, read next
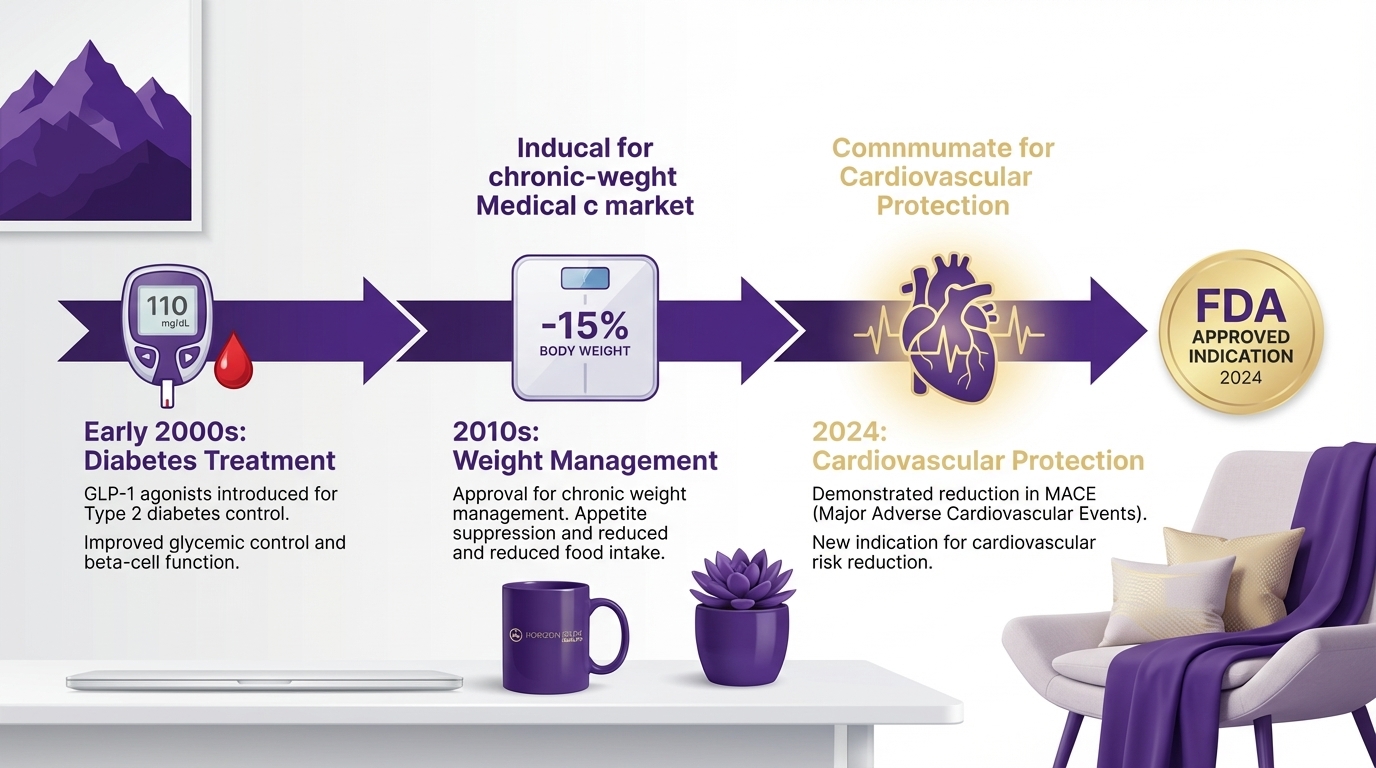
The Evolution of GLP-1 Agonists: From Diabetes Treatment to Cardiovascular Protection
GLP-1 medications used to sit in the diabetes lane.
That lane is gone.
Now the conversation includes obesity, cardiovascular risk, obstructive sleep apnea, liver disease, psychiatric medications that drive weight gain, inflammation, food noise, and long-term maintenance. That does not mean GLP-1s are magic. It means the old way of separating "mental health," "weight," "sleep," and "metabolic disease" looks less useful than it used to.
The Fast Answer
- GLP-1 medications started as diabetes treatments, but the modern clinical role is broader.
- Wegovy has FDA indications for chronic weight management, cardiovascular risk reduction in adults with established cardiovascular disease and overweight/obesity, and noncirrhotic MASH with moderate-to-advanced fibrosis under accelerated approval.
- Zepbound is FDA-approved for chronic weight management and for moderate-to-severe obstructive sleep apnea in adults with obesity.
- The stronger the medications become, the more monitoring matters. Nutrition, lean mass, gallbladder symptoms, pancreatitis symptoms, kidney function, diabetes medication interactions, pregnancy plans, and contraindications all belong in the plan.
- I do not treat GLP-1s as cosmetic medication. I treat them as metabolic-risk medication that needs a real plan.
Before you keep searching
If this answer changes what you might do next, pick the next clinical question now.
The Timeline That Actually Matters
| Era | What Changed | Clinical Meaning |
|---|---|---|
| Diabetes treatment | GLP-1 receptor agonists improved glucose control | The class started as endocrine medicine, not aesthetics |
| Chronic weight management | Higher-dose semaglutide and later tirzepatide changed obesity treatment | Weight loss became large enough to affect multiple risk factors |
| Cardiovascular outcomes | SELECT showed semaglutide reduced major cardiovascular events in adults with CVD and overweight/obesity without diabetes | Weight-management medication crossed into cardiovascular prevention |
| Sleep apnea | Tirzepatide gained an FDA indication for moderate-to-severe OSA in adults with obesity | Sleep became part of the metabolic treatment conversation |
| MASH | Wegovy received accelerated approval for noncirrhotic MASH with moderate-to-advanced fibrosis | Liver disease entered the GLP-1 clinical map |
That is the real evolution. Not a new diet trend. A medication class moving into chronic disease risk.
Why Psychiatry Should Care
Psychiatry does not get to ignore metabolic health.
Many patients arrive with depression, anxiety, ADHD symptoms, fatigue, insomnia, binge eating, antipsychotic-associated weight gain, SSRI-associated weight changes, untreated sleep apnea, insulin resistance, or shame from years of being told to "just try harder."
If the metabolic problem is driving sleep, inflammation, fatigue, and self-esteem, treating only the mood symptoms can miss the center of the case.
But the reverse is also true. If psychiatric medications, trauma, binge eating, ADHD, or sleep deprivation are driving the metabolic pattern, a GLP-1 alone is not enough.
That is why I like diagnostic psychiatry for this work. The medication is only one part of the pattern.
Cardiovascular Protection Was The Turning Point
The SELECT trial changed how clinicians talk about semaglutide.
In adults with established cardiovascular disease and overweight or obesity, without diabetes, semaglutide reduced major adverse cardiovascular events compared with placebo. The FDA then approved Wegovy to reduce the risk of cardiovascular death, heart attack, and stroke in adults with cardiovascular disease and either obesity or overweight.
That approval matters because it moves the drug out of the narrow "weight loss" frame.
For the right patient, I want a better set of questions.
- What is the cardiovascular risk?
- What is already being treated with statins, blood pressure medication, or diabetes prevention?
- What does weight loss change?
- What benefits may be independent of the scale?
- What risks come with treatment?
Weight is part of the story. It is not the entire story.
Tirzepatide Changed Expectations For Weight Loss
Tirzepatide raised the weight-loss bar because it acts on both GIP and GLP-1 receptors. In the 2025 SURMOUNT-5 head-to-head trial, tirzepatide produced greater average weight loss than semaglutide at 72 weeks in adults with obesity but without diabetes.
That is clinically meaningful.
It also creates a monitoring problem. Faster or larger weight loss can expose weak planning.
- not enough protein
- no resistance training
- constipation ignored until it is severe
- nausea treated by barely eating
- muscle loss mistaken for success
- no plan for maintenance
I do not want a patient to become smaller and metabolically fragile.
Sleep Apnea Belongs In The Same Conversation
In December 2024, the FDA approved Zepbound for moderate-to-severe obstructive sleep apnea in adults with obesity, alongside reduced-calorie diet and increased physical activity.
That is a big shift because sleep apnea often masquerades as psychiatric illness.
- brain fog
- low motivation
- irritability
- morning headaches
- anxiety-like awakenings
- depression that does not respond cleanly
- ADHD-like attention problems
If someone is seeking GLP-1 treatment and also has sleep symptoms, I want that evaluated. Treating weight while ignoring oxygen drops at night is not good medicine.
MASH Makes The Liver Part Of The Story
The newer Wegovy labeling includes treatment of noncirrhotic metabolic dysfunction-associated steatohepatitis, or MASH, with moderate-to-advanced fibrosis in adults. The FDA approval is accelerated, which means confirmatory outcome data still matters.
This does not mean every person with fatty liver needs Wegovy. It means GLP-1 therapy is moving deeper into metabolic disease management.
For patients with elevated liver enzymes, insulin resistance, high triglycerides, abdominal weight gain, or known fatty liver disease, I want the metabolic workup to be organized. A medication decision should not happen in isolation from the liver story.
The Safety Screen Is Not Optional
Before GLP-1 or GIP/GLP-1 medication, I want a real safety review.
These are the questions I ask before I am comfortable.
- Any personal or family history of medullary thyroid carcinoma or MEN2?
- Any pancreatitis history?
- Any gallbladder disease or severe abdominal pain episodes?
- Pregnant, trying to conceive, or planning pregnancy?
- Diabetes medications that could cause hypoglycemia?
- Kidney disease or dehydration risk?
- Severe reflux, suspected gastroparesis, or repeated vomiting?
- Planned surgery or anesthesia?
- Restrictive eating, binge eating, or poor protein intake?
- Current psychiatric symptoms, including suicidal thoughts?
The point is not to scare people. The point is to practice like this is medication, because it is.
My Clinical Position
GLP-1s are not a shortcut around clinical thinking.
They are powerful tools for the right patient, especially when metabolic risk, cardiovascular risk, sleep apnea, liver disease, psychiatric medication weight gain, or appetite dysregulation are part of the pattern.
But a premium GLP-1 plan needs more than a prescription.
- baseline medical history and labs
- side-effect prevention
- protein and resistance training
- sleep screening
- medication interaction review
- realistic maintenance planning
- clear stop-and-call instructions
I am not impressed by fast weight loss if the patient is nauseated, dehydrated, constipated, losing strength, and afraid to eat.
I am impressed by weight loss that comes with better blood pressure, better sleep, better labs, preserved function, and a plan the patient can live with.
Considering GLP-1 Therapy?
At Horizon Peak Health, GLP-1 discussions are part of a broader diagnostic evaluation. We look at metabolic risk, psychiatric medication history, sleep, nutrition, labs, contraindications, and treatment goals before deciding whether medication makes sense.
Bring the medication list. Bring the labs. Bring the sleep symptoms. Bring the part of the story that has never been connected.
Book a diagnostic consultation
Locations: Psychiatric evaluation in Rancho Palos Verdes, Psychiatric evaluation in Phoenix, Psychiatric evaluation in Chandler, and telehealth throughout California and Arizona.
References
- FDA. (2024). FDA approves first treatment to reduce risk of serious heart problems specifically in adults with obesity or overweight.
- FDA. (2024). FDA approves first medication for obstructive sleep apnea.
- FDA. (2025). FDA approves treatment for serious liver disease known as MASH.
- DailyMed. WEGOVY prescribing information.
- DailyMed. ZEPBOUND prescribing information.
- Lincoff, A. M., Brown-Frandsen, K., Colhoun, H. M., et al. (2023). Semaglutide and cardiovascular outcomes in obesity without diabetes. New England Journal of Medicine.
- Aronne, L. J., Horn, D. B., le Roux, C. W., et al. (2025). Tirzepatide as compared with semaglutide for the treatment of obesity. New England Journal of Medicine.
Medical Disclaimer: This article is for educational purposes only and does not constitute medical advice. GLP-1 medications are prescription treatments with specific indications, contraindications, and monitoring needs. Treatment decisions should be made with a qualified healthcare provider who can evaluate your cardiovascular risk, diabetes medications, pregnancy plans, kidney function, gallbladder history, pancreatitis history, family or personal history of medullary thyroid carcinoma or MEN2, nutrition status, and lean-mass risk. Seek urgent medical care for severe or persistent abdominal pain, repeated vomiting, dehydration, fainting, signs of hypoglycemia, or another medical emergency. Do not start, stop, or change these medications without medical supervision.
If suicidal thoughts show up while you are considering or using a GLP-1, treat that as a safety signal, not something to watch alone. If you might hurt yourself or cannot stay safe, call or text 988 for the Suicide and Crisis Lifeline or go to emergency care. If the thoughts are present but you are safe right now, talk to your prescriber before starting, increasing, stopping, or restarting the medication.
Written by
Canybec Sulayman APRN, PMHNP-BC, CCRN-CSC
Investigating the root causes of mental health symptoms with 19 years of ICU diagnostic rigor.
Want a plan that fits the whole picture?
Bring the symptoms, medication history, labs, sleep pattern, and questions. The goal is a clearer explanation and safer next step.
